Rapid Analysis of Clozapine and Norclozapine in Plasma for Clinical Research
연구용으로만 사용되며 진단 절차에는 사용할 수 없습니다.
Abstract
Large-scale pharmacokinetic and population studies, benefit from the availability of robust, and high-throughput analytical procedures. Here we describe a method suitable for clinical research settings which uses a simple and inexpensive preparation technique using relatively little sample. This is followed by the quantification of clozapine and norclozapine using liquid chromatography and tandem mass spectrometry.
Benefits
- Short analytical run time (72 sec per sample) and high throughput capability
- Analytical selectivity afforded by chromatography and mass detection
- Simple and inexpensive preparation using low sample volumes
Introduction
Large-scale pharmacokinetic and population studies, are likely to benefit from the availability of robust and high-throughput analytical procedures.
Here we describe a method suitable for clinical research which involves the precipitation of human plasma proteins using an internal standard in acetonitrile, followed by the quantification of clozapine and norclozapine using liquid chromatography and tandem mass spectrometry.
Chromatographic elution was completed in 42 seconds with an injection-injection time of 72 seconds using a Waters™ XBridge™ Premier BEH™ C18 Column on the ACQUITY UPLC™ I-Class Flow Through Needle system. Analytes were detected by multiple reaction monitoring (MRM) on a Xevo™ TQ-S micro Mass Spectrometer (Figure 1).
 Figure 1. ACQUITY UPLC I-Class System and a Xevo TQ-S micro Mass Spectrometer.
Figure 1. ACQUITY UPLC I-Class System and a Xevo TQ-S micro Mass Spectrometer.
Experimental
Sample Preparation
Plasma calibrators and quality control materials were prepared using pooled human plasma supplied by BioIVT (West Sussex, United Kingdom). Concentrated stock solutions were prepared from certified powders of clozapine, norclozapine, and deuterium-labelled clozapine as an internal standard, supplied by Toronto Research Chemicals (Ontario, Canada). The calibration range was 50–2000 ng/mL for both analytes.
Sample Extraction
A three-fold volume excess of internal standard (2H4-clozapine in acetonitrile) was added to 50 µL of sample in a microcentrifuge tube. Tubes were agitated on a multi-tube vortex mixer at 2000 r.p.m. for one minute, and then centrifuged at room temperature, for five minutes at 16200 x g. Twenty microliters of supernatant was transferred to a 2 mL 96-well plate, and 450 µL of 30% (v/v) methanol (aq) was added.
UPLC Conditions
|
System: |
ACQUITY UPLC I-Class with Flow Through Needle (FTN) |
|
Needle: |
30 µL |
|
UPLC column: |
XBridge Premier BEH C18 UPLC, 2.5 µm particle, 2.1 x 50 mm internal diameter (p/n: 186009827) |
|
Inline column filter: |
XBridge Premier BEH C18 UPLC, 2.5 µm particle, 2.1 x 5 mm VanGuard™ FIT cartridge (p/n: 186009842) |
|
Mobile phase (A): |
5 mM Ammonium formate in 0.1% (v/v) formic acid (aqueous) |
|
Mobile phase (B): |
5 mM Ammonium formate in 0.1% (v/v) formic acid in 80/20 (v/v) solution of methanol/isopropanol |
|
Needle wash solvent: |
0.1% (v/v) formic acid in 1/1/1/1 (v/v) solution of methanol/acetonitrile/isopropanol/water |
|
Purge solvent: |
30% (v/v) Methanol (aqueous) |
|
Seal wash: |
As for Purge Solvent |
|
Column temperature: |
45 °C |
|
Injection volume: |
2 µL |
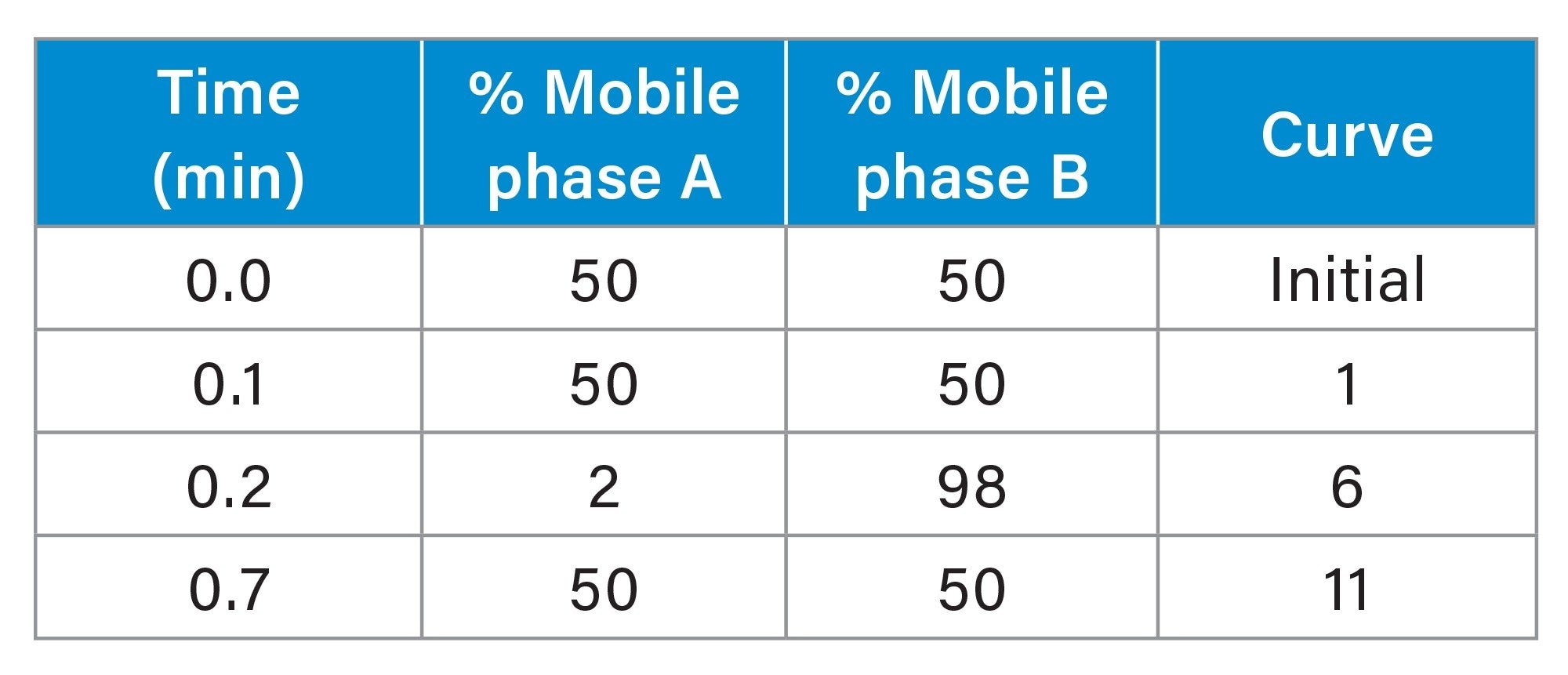 Table 1. Binary solvent manager gradient table.
Table 1. Binary solvent manager gradient table.
|
Flow rate: |
0.6 mL/min |
|
Run time: |
0.7 mins (1.2 minutes injection-injection) |
MS Conditions
|
System: |
Xevo TQ-S micro |
|
Quadrupole resolution: |
MS1 and MS2 at 0.7 Full Width Half Maximum (0.6–0.8 acceptable) |
|
Acquisition mode: |
Multiple Reaction Monitoring (MRM) (See Table) |
|
Method events: |
Divert to MS Waste <0.2 minute and >0.5 minute |
|
Polarity: |
Electrospray Positive Ionization |
|
Capillary: |
3.00 kV |
|
Source temperature: |
150 °C |
|
Desolvation temperature: |
600 °C |
|
Desolvation gas flow: |
1000 L/Hr |
|
Cone gas flow: |
25 L/Hr |
|
Inter-Channel, -Scan and polarity switch delay: |
Automatic |
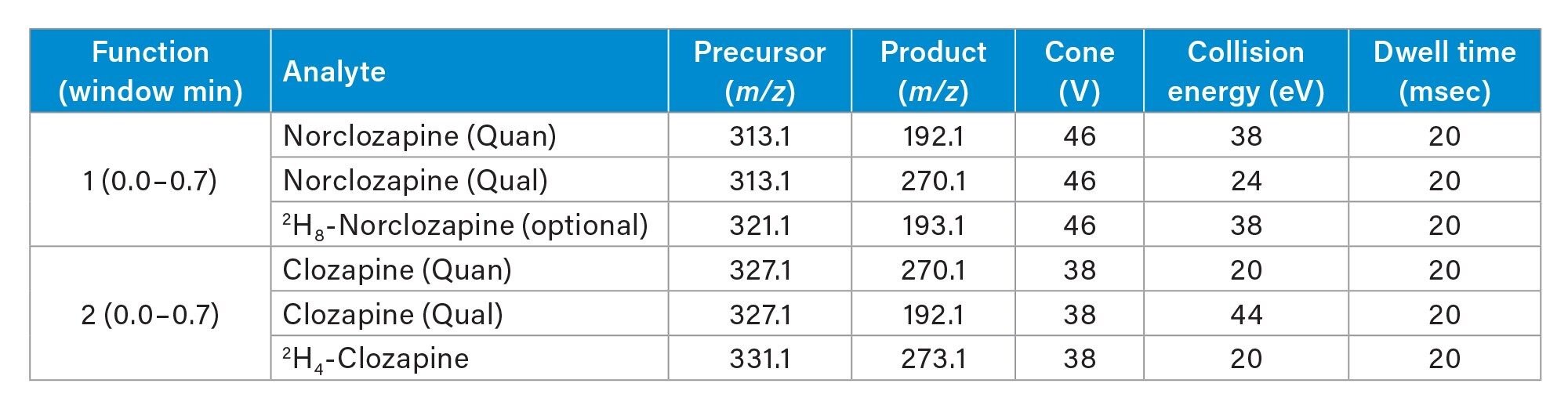 Table 2. Multiple reaction monitoring ion transitions.
Table 2. Multiple reaction monitoring ion transitions.
|
Data management: |
MassLynx™ v4.2 with TargetLynx™ Application Manager |
Results and Discussion
Table 3. summarizes the performance characteristics of the developed method, demonstrating excellent imprecision and bias performance.
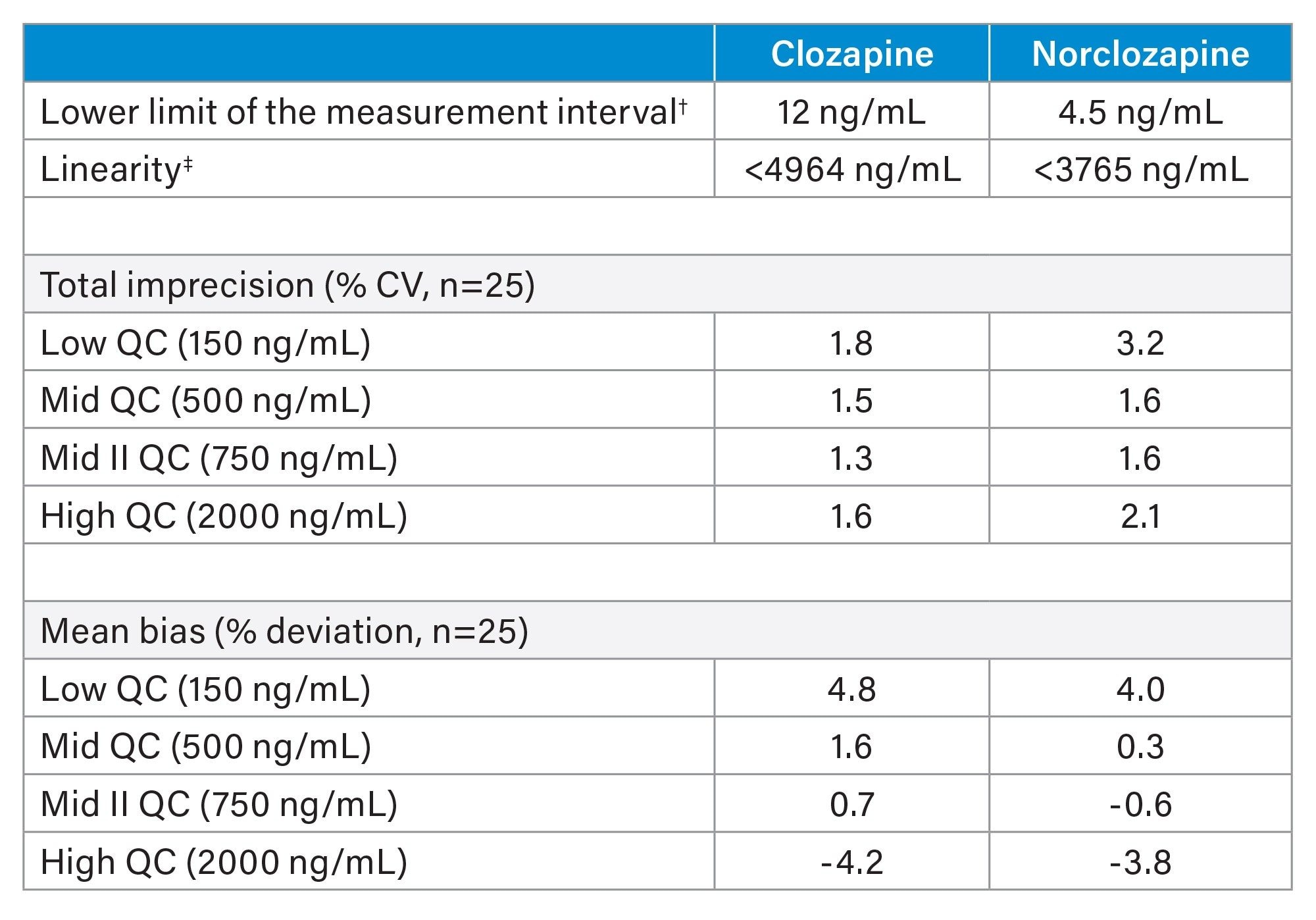 Table 3. Performance summary.
Table 3. Performance summary. † Lowest nominal concentration measurable with ≤20% imprecision (relative standard deviation (RSD) and ≤15% deviation from nominal concentration.
‡ No significant 2nd or 3rd order polynomial terms (p<0.05) and r2 ≥0.997.
Using wash solvents and mobile phases with high organic solvent content ensured carryover was negligible (<25% of the LLMI) as evidenced when blank samples were analysed in sequence with high concentration samples (~2-times the upper-most calibrator concentration, n=10 each condition, data not shown).
The combination of sample dilution, low injection volume and diversion of LC eluant to waste allowed for stable chromatographic separation and quantification of clozapine and norclozapine, with retention deviating by no more than 0.36 seconds from the expected retention time, and measured concentration varying by no more than 1.2% (RSD) (Figure 2).
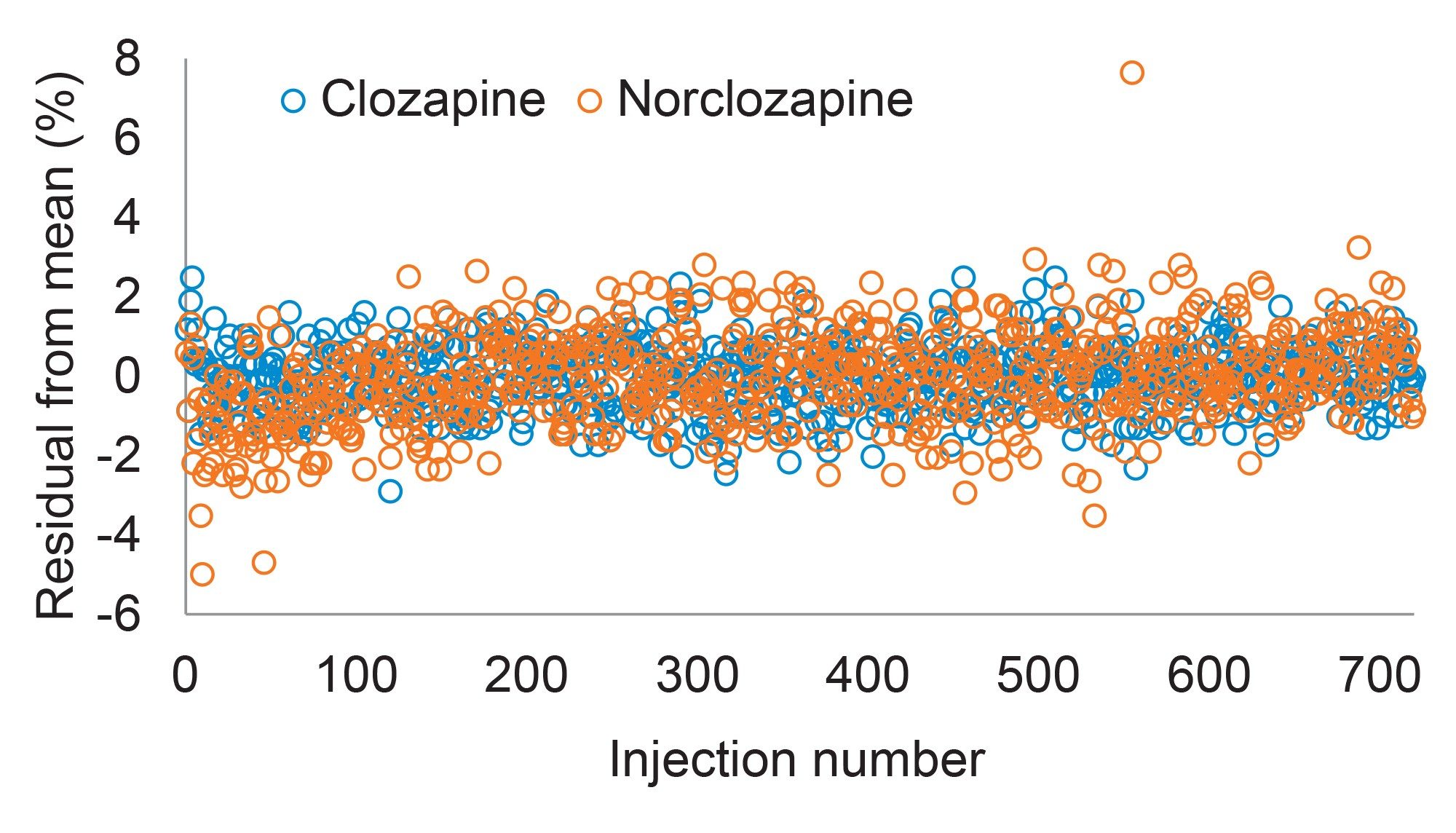 Figure 2. Quantification of clozapine and norclozapine over 14 hours of continuous operation shows detector stability for extended periods of analysis. Mean concentration and measurement imprecision (%RSD) of clozapine in the pooled sample was 688 ng/mL (0.8%) and 680 ng/mL (1.2%) for norclozapine, n=720.
Figure 2. Quantification of clozapine and norclozapine over 14 hours of continuous operation shows detector stability for extended periods of analysis. Mean concentration and measurement imprecision (%RSD) of clozapine in the pooled sample was 688 ng/mL (0.8%) and 680 ng/mL (1.2%) for norclozapine, n=720.
Clozapine and norclozapine co-eluted (Figure 3) in a step gradient where the organic solvent content of the flow solvent increased by 48% over six seconds. Co-elution gave the opportunity to evaluate the use of a single internal standard for quantification of both compounds.
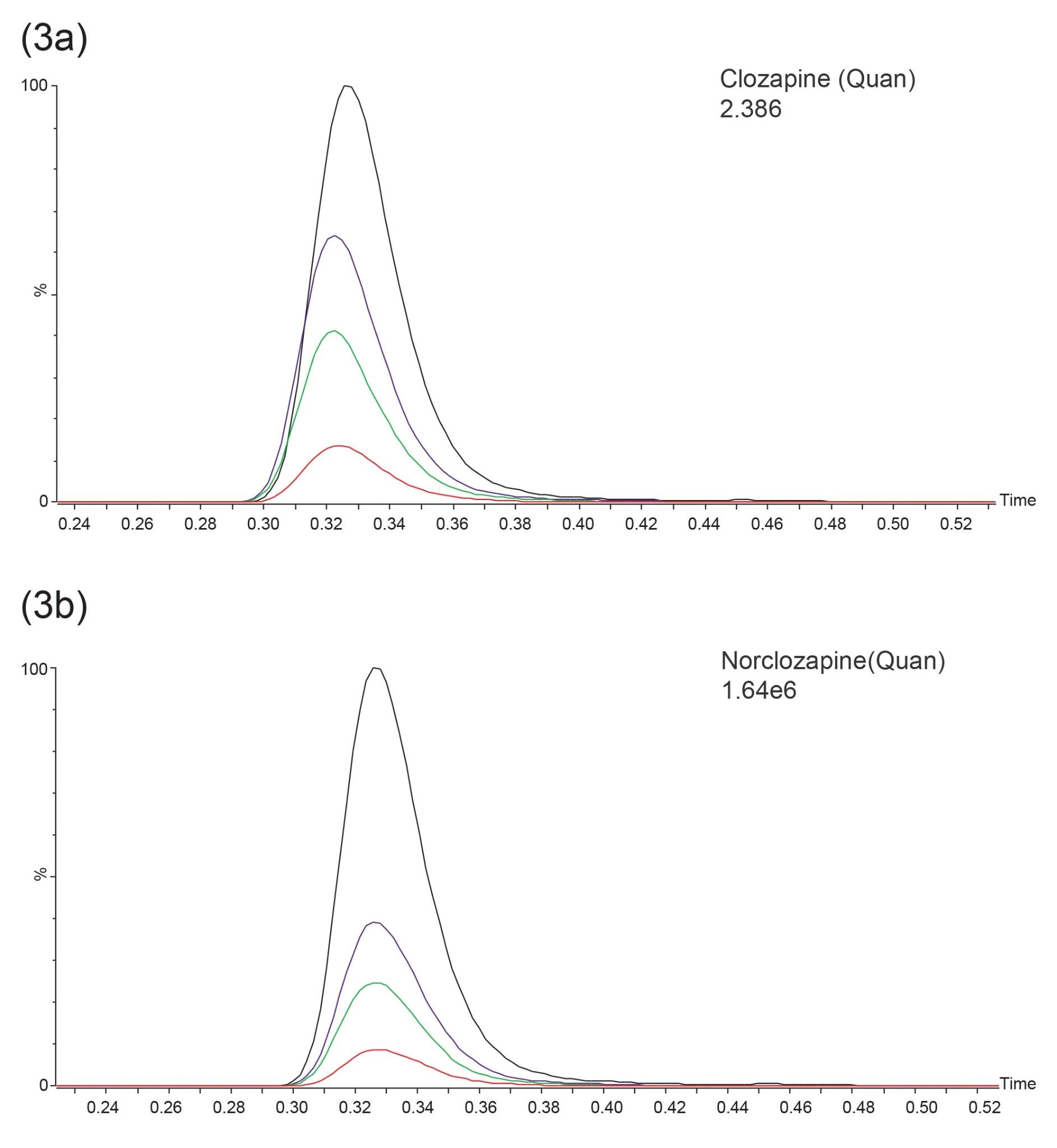 Figure 3. Representative smoothed MRM quantifier ion transition chromatograms of clozapine (a) and norclozapine (b) in the internal quality control samples. Target / nominal control concentrations: 150 ng/mL (red), 500 ng/mL (green), 750 ng/mL (purple), and 2000 ng/mL (black).
Figure 3. Representative smoothed MRM quantifier ion transition chromatograms of clozapine (a) and norclozapine (b) in the internal quality control samples. Target / nominal control concentrations: 150 ng/mL (red), 500 ng/mL (green), 750 ng/mL (purple), and 2000 ng/mL (black).
Analyte: internal standard peak area response ratios for clozapine extracted from plasma were between 98.2 and 101.7% (mean 100.3%, n=6) of those from solvent standards of equivalent concentration, and between 101.9 and 105.5% (mean 104.1%, n=6) for norclozapine. Residual sample matrix changed the response ratio by no more than 5.5% which is less than the maximum allowable error of ≤10% bias, indicating 2H4-clozapine performs sufficiently not only for clozapine, but also as a surrogate internal standard for norclozapine quantification.
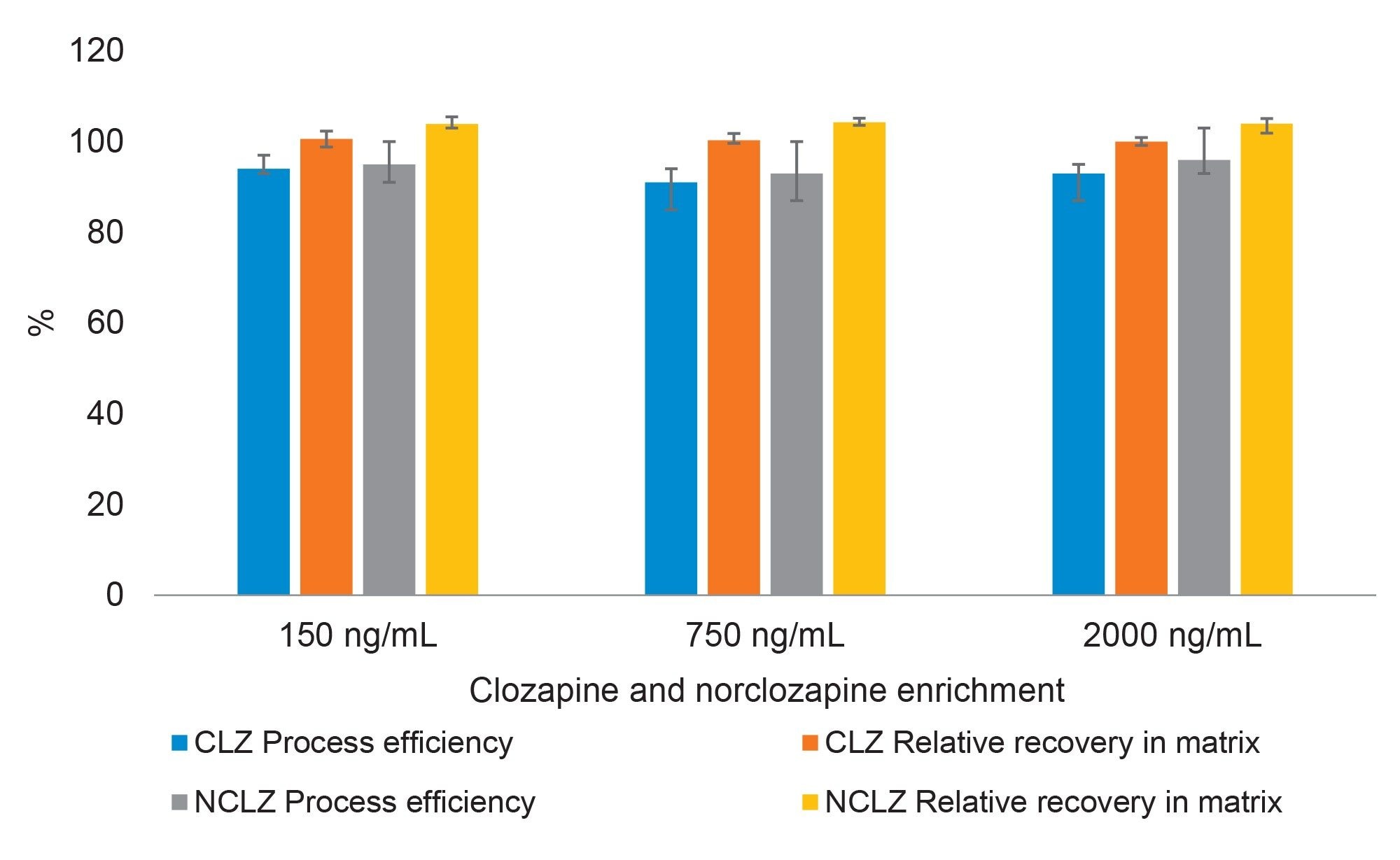 Figure 4. Mean process efficiency and matrix effects for clozapine and norclozapine using plasma samples from six healthy adult blood donors, measured in triplicate at each level. Process efficiency is the pre-extraction spiked sample analyte: internal standard peak area response, normalized to the post-extraction spiked response. The relative recovery in matrix is the post-extraction spiked sample response, normalized to a matrix-free solvent standard of the same concentration (error bars represent range of results).
Figure 4. Mean process efficiency and matrix effects for clozapine and norclozapine using plasma samples from six healthy adult blood donors, measured in triplicate at each level. Process efficiency is the pre-extraction spiked sample analyte: internal standard peak area response, normalized to the post-extraction spiked response. The relative recovery in matrix is the post-extraction spiked sample response, normalized to a matrix-free solvent standard of the same concentration (error bars represent range of results).
Analysis of LGC Axio EQA samples TM230 to TM240, inclusive (n=11), covering the concentration range 118–2210 ng/mL for clozapine and 94–2300 ng/mL for norclozapine, showed good analytical performance. The mean (range) z-scores for were 0.48 (-0.35 to 0.97) for clozapine and 0.33 (-0.21 to 0.67) for norclozapine, with scheme satisfactory performance criteria being a z-score ≤2.00. Bland-Altman analysis showed a mean difference between the developed method and assigned values of <5% for both drugs.
The relationship between the developed (test) and a comparator LC-MS method was described as Test Clozapine (ng/mL) = -10.0 + 0.996 x Comparator Clozapine (ng/mL) and Test Norclozapine (ng/mL) = -8.5 + 0.996 x Comparator Norclozapine (ng/mL), n= 76 samples ranging 0–1003 ng/mL clozapine, and 0–539 ng/mL norclozapine. There was no suggestion of a proportional bias for either analyte, with slopes (95% confidence interval) of 0.996 (0.977–1.016) for clozapine and 0.996 (0.972–1.018) for norclozapine described by Passing-Bablok analysis. A constant negative bias (95% confidence interval) was found in the test method of 10 ng/mL (5–18) for clozapine and 9 ng/mL (5–13 ng/mL) for norclozapine. This is possibly explained by differences in method calibration and sample instability.
The analytical selectivity of the MRM ion transitions was confirmed by inspecting chromatograms of injected solvent standards of candidate interfering substances. No peak or chromatogram baseline interferences were noted around the clozapine or norclozapine retention time (0.32 min) when the following standard solutions in 30% (v/v) methanol (aq) were injected using the described LC and MS/MS methods: 20 ng/mL amitriptyline, clomipramine, doxepine, imipramine, maprotiline, norclomipramine, desipramine, nordoxepine, normaprotiline, nortrimipramine, nortriptaline, protriptaline, trimipramine; 25 ng/mL temazepam, triazolam, midazolam, oxazepam, clonazepam, flurazepam, chlordiazepam, clobazam, diazepam, and lorazepam; 100 ng/mL citalopram, desmethylfluoxetime, duloxetine, fluoxetine, O-desmethylvenlafaxine, sertraline, and venlafaxine; 50 ng/mL mirtazapine and 300 ng/mL trazodone. Using a maximum acceptable peak area of 35 and 205 counts for norclozapine and clozapine channels, respectively (approximate peak area expected at 25% of the lower limit of the measuring interval), no interfering peaks were seen (data not shown), suggesting the tested compounds would be unlikely to interfere with the integration and subsequent quantitation of target analytes.
In addition, a selection of endogenous compounds were added to clozapine and norclozapine control samples to evaluate potential interference with the overall recovery of clozapine and norclozapine. The nominal concentrations of clozapine/norclozapine were 150 ng/ml (low) and 2000 ng/mL (high). Recovery was reduced by no more than 5.4% in the presence of candidate interferences (n=3 each set of controls). The quantification of clozapine and norclozapine is unlikely to be affected by changes in the levels of the endogenous compounds tested (albumin, cholesterol, triglycerides, bilirubin, uric acid, or creatinine).
Conclusion
A simple clinical research method for the rapid quantification of clozapine and norclozapine in plasma samples with excellent analytical performance characteristics was developed.
720008286, March 2024